
Abstract
Double little toenails, or accessory nails of the fifth toe, are a rare and particular deformity distinct from other nail dysplasias. We describe 4 cases of female patients, including a 6-year-old girl, experiencing this bilateral condition after birth. The nail anomaly shows an autosomal-dominant type of transmission that affects only female individuals. The subjects examined were from a family without marriages between blood relatives and without neuroectodermal hereditary diseases. The 4 patients had no bone alterations of the terminal phalanges of the fifth toe or alterations of the joints of the toes or hair. One patient had nail deformity associated with epilepsy; another patient, associated with an infection of an accessory nail.
Key words: double little toenail, ectopic nail, hereditary accessory nail of the fifth toe, nail morphology, onychodysplasia, split nail
Introduction
The diagnostic criteria of the double nail of the fifth toe, its differential diagnosis with the true ectopic nail, the possible pathogenesis, and surgical treatment are illustrated. We believe that this condition occurred in a particular location as a clinical variant of the congenital ectopic nail because of a late mutation.
Case report
Double little toenails, or inherited accessory nail of the fifth toe, are a rare onychodysplasia with variable genetic expression.1 Nevertheless, few cases of this condition in family members are reported in the literature.2 Here, we describe this nail defect observed in 4 female members of a family.
A 26-year-old woman was evaluated for 2 hyperkeratotic prominences located on the lateral fifth toe surfaces of the main nail (Fig 1A and B). These accessory nails had arisen and grown at the same rate as the normal nail. This condition was causing slight pain during walking, and the patient also expressed concern about a cosmetic disfigurement. Her 34-year-old sister (Fig 1C and D) and her 54-year-old mother have had the same abnormality since childhood. The 6-year-old girl, who was the proband's niece, has had this deformity since aged 3 years. The family was composed of 20 members in 3 generations (Fig 2, A).
Fig 1.
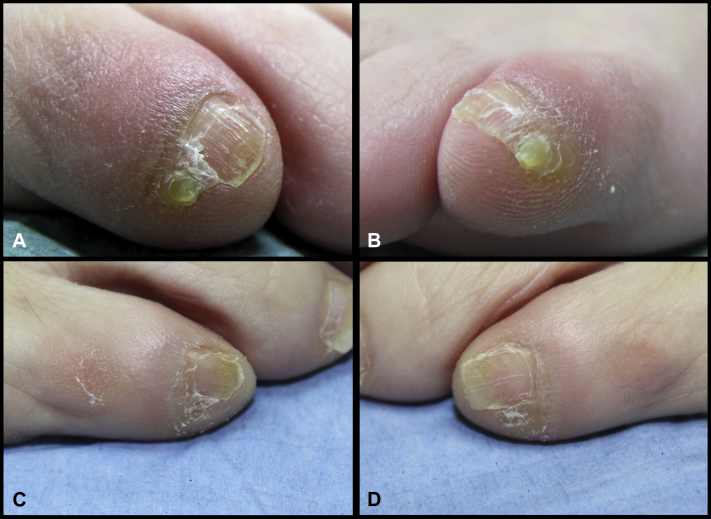
Clinical presentation of double little toenail of the fifth toe in the proband (A, B). Clinical feature of the double little toenail of the fifth toe in the older sister of the proband (C, D).
Fig 2.
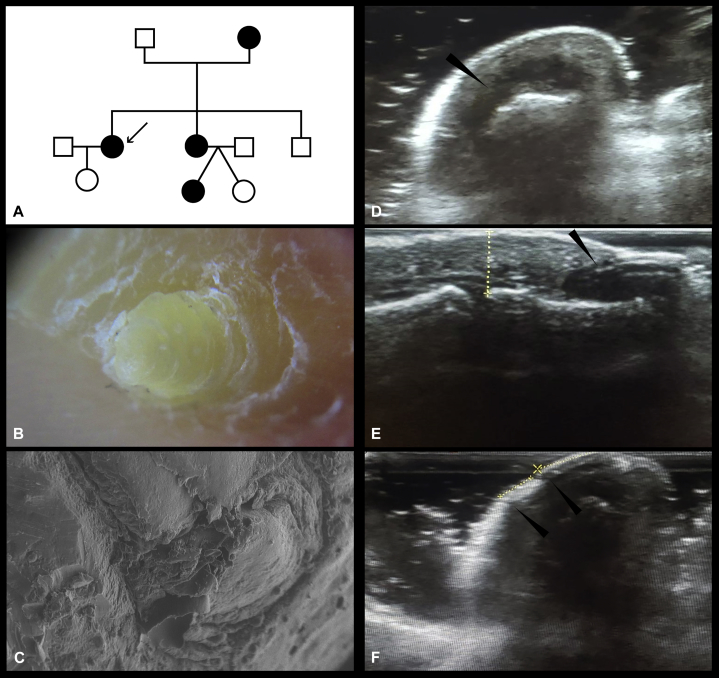
A, Short pedigree of the affected family with double little toenail of the fifth toes. B, Dermoscopic features of the accessory nail of the fifth toe, resembling staves of a barrel (similar to the ectopic nail). C, Scanning electron microscopy image of the double little toenail, showing a stumpy nail with vertical groove, nail folds, and hyponychium. D to F, Echotomography of the nail of the fifth toe of the right foot of the proband. D, Coronal section below the eponychium, showing a hypoechoic area corresponding to the supernumerary nail matrix, 2 mm in diameter; this area seems separated from the main matrix of the nail by an isthmus. E, Longitudinal side section showing the accessory nail plate equipped with a nail bed above the bone phalanx, with a hypoechoic area of approximately 1.7 mm, which corresponds to its matrix. F, Coronal section in a distal position showing the 2.5-mm-wide accessory nail plate of the double little toenail, separated by a thin groove from the main plate.
The patients did not report any history of trauma to the foot. The older sister had a staphylococcal infection in one of the abnormal toenails. All patients were healthy and had no skeletal, hair, or tooth abnormalities. The proband had been treated for epilepsy and had paroxysmal tachycardia. The examination showed that these nails, in addition to being small compared with the main nail, were separated from it by a vertical groove that departed from the cuticle up to the hyponychium. These were grayish yellow and the perionychium appeared normal. Dermoscopy of these nails highlighted a proximal fold, lateral nail fold, and the hyponychium. The size varied between 3 and 6 mm in diameter at the base and 4 and 7 mm long. Moreover, some accessory toenails showed a pattern with transverse bands and grooves that were reminiscent of staves of a barrel (Fig 2, B).
Superficial texture of accessory toenails was reproduced by a silicone cast technique. Its analysis by scanning electron microscopy showed a shrunken and stumpy nail with a wrinkled surface (Fig 2, C). Ultrasonography of the fifth toe showed 2 distinct nail plates with 2 matrices, 1 main and a smaller connected one located more laterally. The latter, which is the basis of the double little toenail, appears as a hypoechoic area connected by an offshoot or isthmus to the primary nail matrix portion in an intermediate position (Fig 2D–F). No abnormalities were observed in karyotype analysis. The radiograph of the feet and the distal phalanx did not show any bone abnormalities. We diagnosed this nail defect according to morphologic criteria as double little toenails. One patient was treated with cryotherapy, followed by the application of a phenol solution. A recurrence was observed 2 years later. The follow-up is 7 years.
Discussion
The double little toenail was first described more than 50 years ago.3 This defect occurs at birth or in childhood, and rarely in adulthood. It is congenital or acquired, with sporadic appearance.4 Histologically, it is similar to nail tissue with a matrix and nail bed, adjacent to the primary toenail. This disorder appears hereditary and it can be observed in both sexes but prevails in the female sex. In the family we discuss, the nail disorder has an autosomal dominant trait. Clinically, the double little toenail develops adjacent to and partly overlapping the plate of the leading nail. The nail, apparently divided into 2 parts by an intermediate furrow, is visible. Congenital double little toenail shows a symmetry in both locations on the fifth toes, although one-fourth of these abnormal nails show a more marked picture on 1 side, as in 2 of our patients. A Y-shaped radiologic alteration of the distal phalanx was occasionally detected; this feature is similar to a hexadactyly.5 Indeed, a macronychia of the fifth toe with accessory double nail was observed as polydactyly.6 A case of double nail developing on the middle finger was recently described.7
Double little toenail must be distinguished from the ectopic nail, acquired split nail, cutaneous horn, and nail fibrokeratoma. Ectopic nails of the feet are unusual.8 The morphology of the newly formed nails shows close similarities with the ectopic nail but differs from this for the site and heredity. The classification of ectopic nail9 includes nail with accessory finger or polydactyly, dorsal and double nail, and a small nail located near the healthy toenail. The latter type includes the double little toenail. Onychoheterotopia is adjacent to but detached from the primary nail, unlike inherited double little toenail, in which the nail is attached to the primary nail. Similarities between the double little toenail and the ectopic nail are as follows: they arise spontaneously or after a trauma, they grow more slowly than usual, and they can recur after incomplete avulsion. The double little toenail shows a matrix and a horizontal-parallel growth pattern. The ectopic nail is equipped with a matrix in the center or the back, with a horizontal-vertical growth pattern and a distal or inverted orientation. Scanning electron microscopy is used for analyzing the ectopic nail, identifying the morphologic aspects, and distinguishing from other periungual epithelial neoformations of the foot.10
We suggest the following criteria for the diagnosis of double little toenail:
-
1.
Fifth toe involvement
-
2.
Congenital occurrence
-
3.
Often bilateral
-
4.
Possible hereditary involvement
It seems likely that double little toenail is linked to a variation in the normal genes controlling healthy nail growth and orientation. The pathomechanism is thought to be due to an incomplete development of the primary nail epithelium and onychodermis. In congenital occurrence, misdevelopment may started because the germinal matrix splits, leading to implantation of a fragment proximally into the nail fold. In our patients, we suspected congenital occurrence because the double little toenail matrix appears as an extroflexion or extension to the primary nail matrix at the intermediate lamina. These aspects led us to consider double little toenail as a form of the condition known as congenital onychoheterotopia. The treatment is segmental excision or phenolization. Cryotherapy followed by matrix phenolization is a second-choice treatment.
In conclusion, the double little toenail shows essential aspects in dermoscopy and scanning electron microscopy similar to those of the ectopic nail. We believe that this nail anomaly is unique and represents a clinical variant of ectopic nail.
Footnotes
Funding sources: None.
Conflicts of interest: None disclosed.
References
- 1.Baran R. Double little toenail (inherited accessory nail of fifth toes) In: Baran R., Hadj-Rabia S., Silverman R., editors. Pediatric Nail Disorders. CRC Press; Boca Raton: 2017. p. 27. [Google Scholar]
- 2.Chi C.C., Wang S.H. Inherited accessory nail of the fifth toe cured by surgical matricectomy. Dermatol Surg. 2004;30:177–179. doi: 10.1111/j.1524-4725.2004.30351.x. [DOI] [PubMed] [Google Scholar]
- 3.Hundeiker M. Hereditäre Nageldysplasie der Zehe. Hautarzt. 1969;20:281–282. [PubMed] [Google Scholar]
- 4.Zaouak A., Boufarguine S., Hammmami H., Fenniche S. A tale of a double-nailed toe. Skin Appendage Disord. 2018;3:1–2. doi: 10.1159/000493402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Haneke E. Double nail of the fifth toes. Skin Appendage Disord. 2015;1:163–167. doi: 10.1159/000443378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cannata G.E. Congenital onychodystrophy. Clin Exp Dermatol. 1991;16:75–76. doi: 10.1111/j.1365-2230.1991.tb00309.x. [DOI] [PubMed] [Google Scholar]
- 7.Randhawa M.A., Hussain S., Bilal M. A unique case of accessory/double middle finger. Int J Surg Case Rep. 2018;44:103–104. doi: 10.1016/j.ijscr.2018.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ena P., Ena L., Ferrari M., Mazzarello V. Ectopic nails: clinical and dermoscopic features, treatment and outcome in 20 cases. Dermatology. 2015;231:298–303. doi: 10.1159/000437364. [DOI] [PubMed] [Google Scholar]
- 9.Muraoka M., Yoshioka N., Hyodo T. A case of double finger nail and ectopic fingernail. Ann Plast Surg. 1996;36:201–205. doi: 10.1097/00000637-199602000-00019. [DOI] [PubMed] [Google Scholar]
- 10.Mazzarello V., Ena P., Dessy L.A. A morphological study of ectopic plantar nail. Am J Dermatopathol. 2005;27:122–125. doi: 10.1097/01.dad.0000154394.37842.ae. [DOI] [PubMed] [Google Scholar]


