Lũ mèo với nhiều biểu cảm khác nhau luôn là đề tài chế ảnh hấp dẫn. Vô tình chúng ta chụp lại được một khoảnh khắc hài hước của chúng hoặc ghi lại những video mà chúng thể hiện biểu cảm của mình.
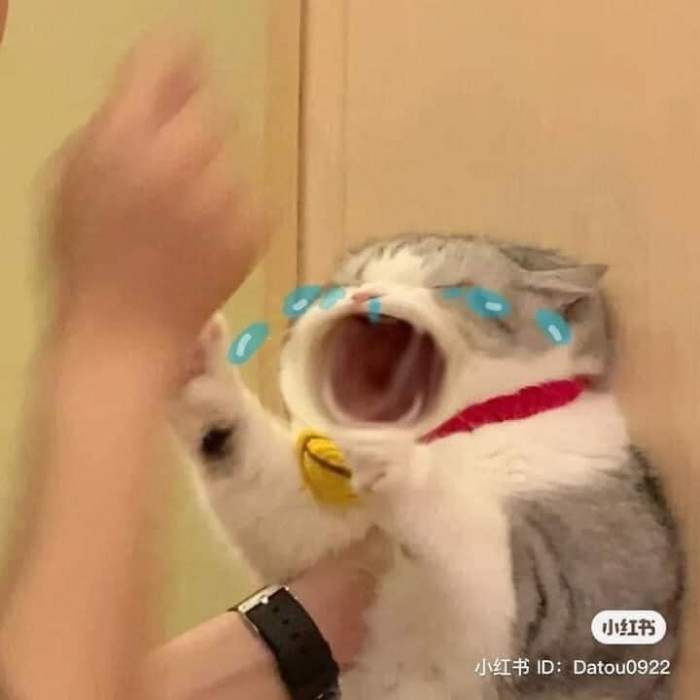
Chúng ta có thể cắt chúng ra từ video và sau đó thì thêm vào đó vài nét vẽ hoặc chữ và có một meme mèo ngon lành. Các thể loại meme như meme mèo hài hước, meme mèo tức giận, meme mèo khinh bỉ,v.v. Rất nhiều các thể loại meme mà bạn có thể chế ra dựa vào biểu cảm của lũ mèo này.
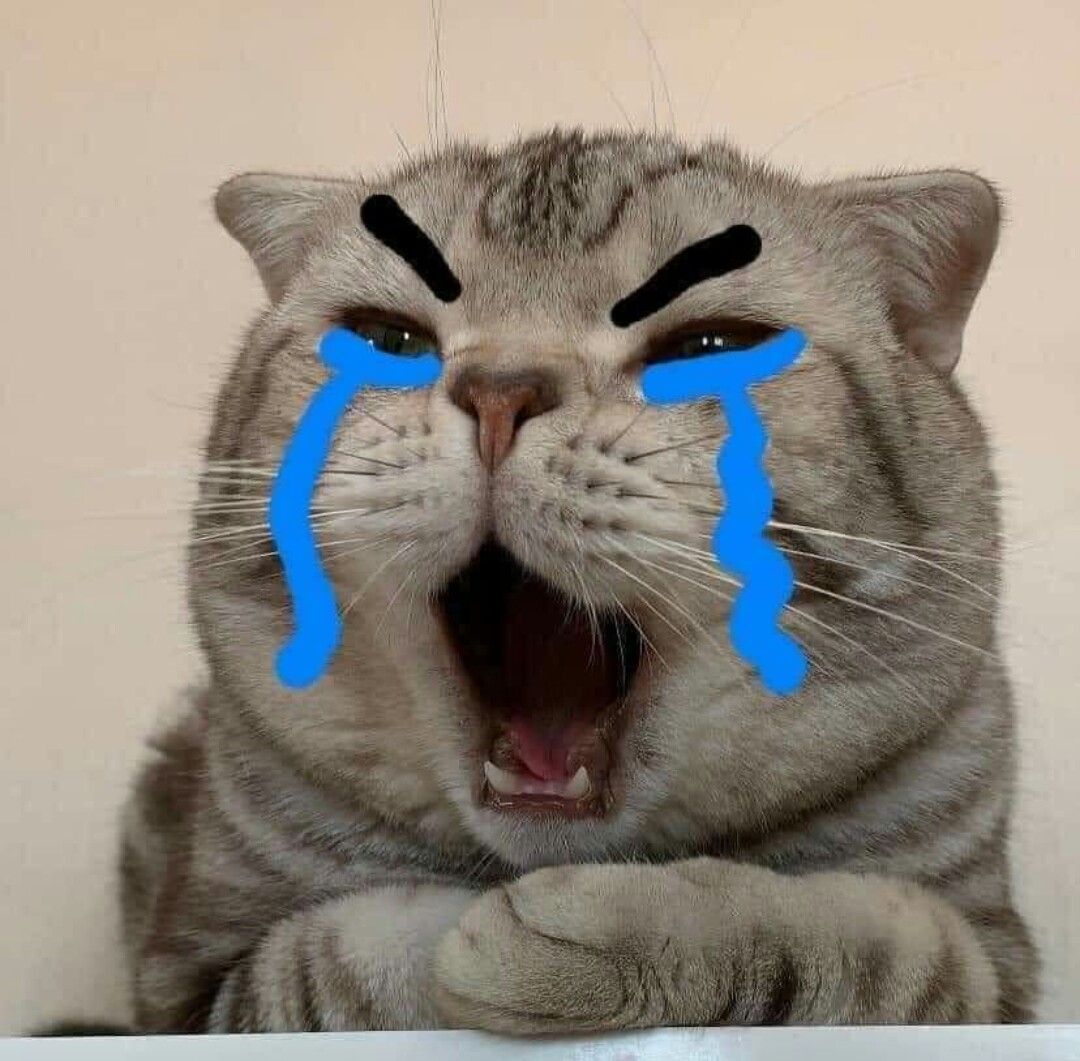
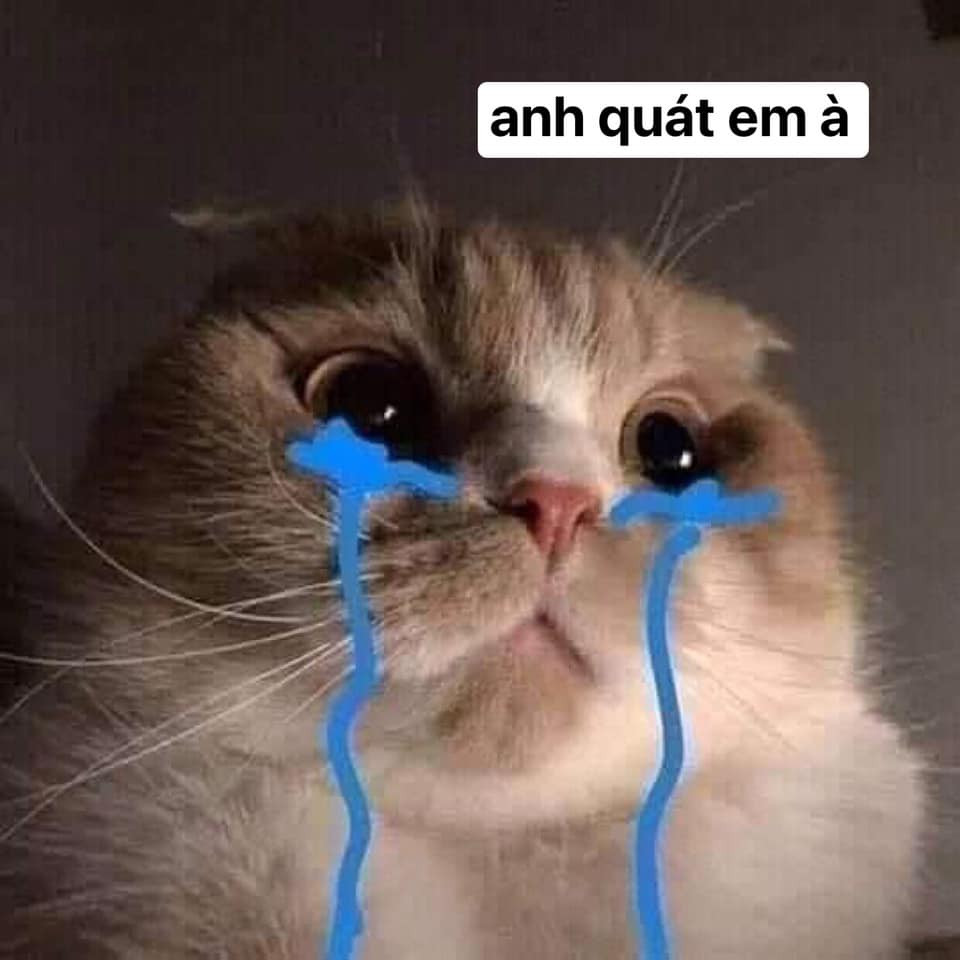
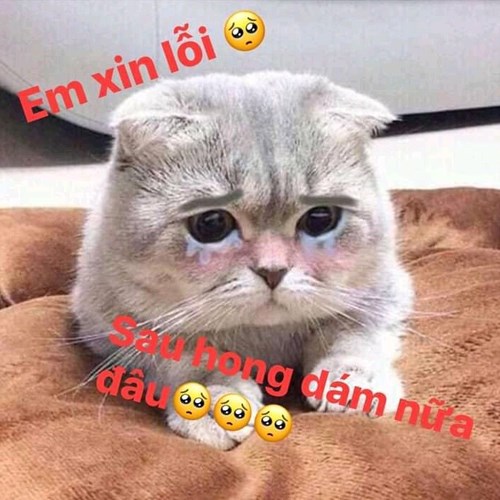
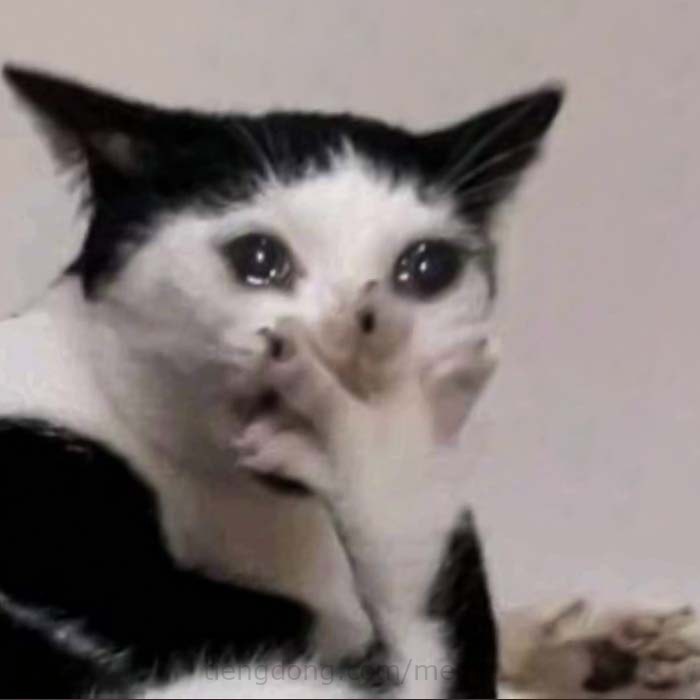
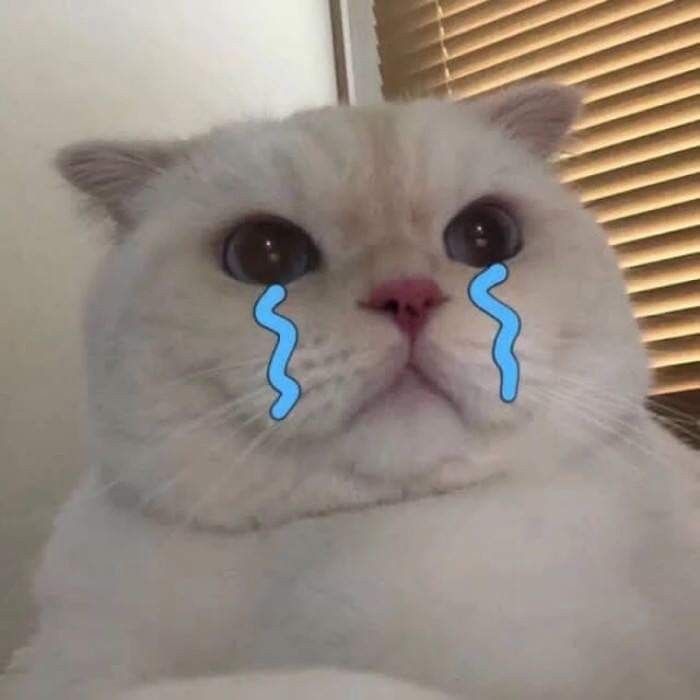
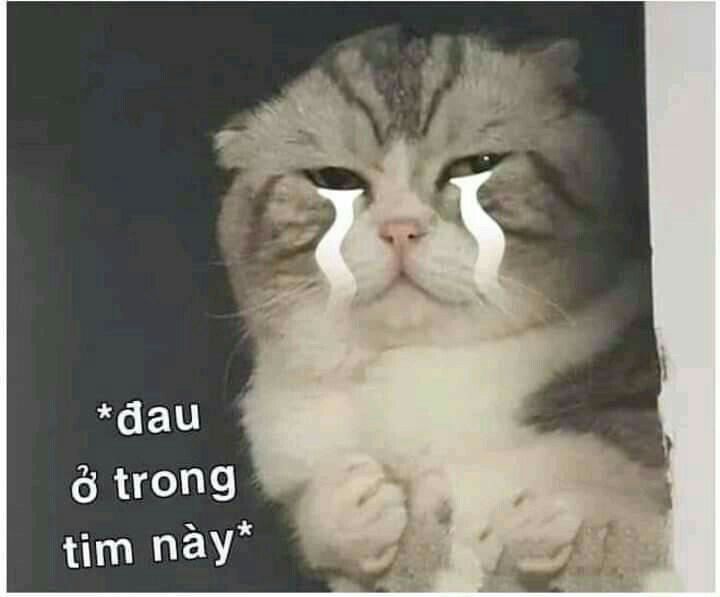
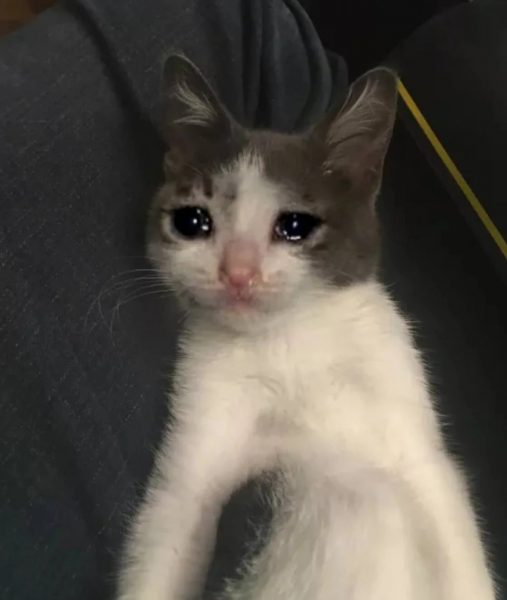
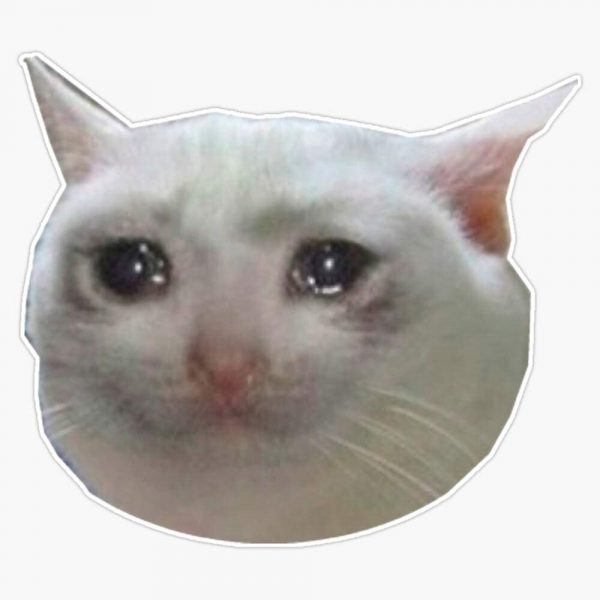
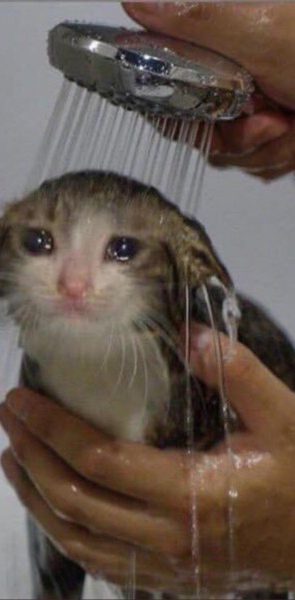
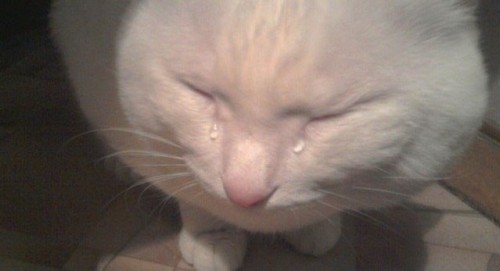
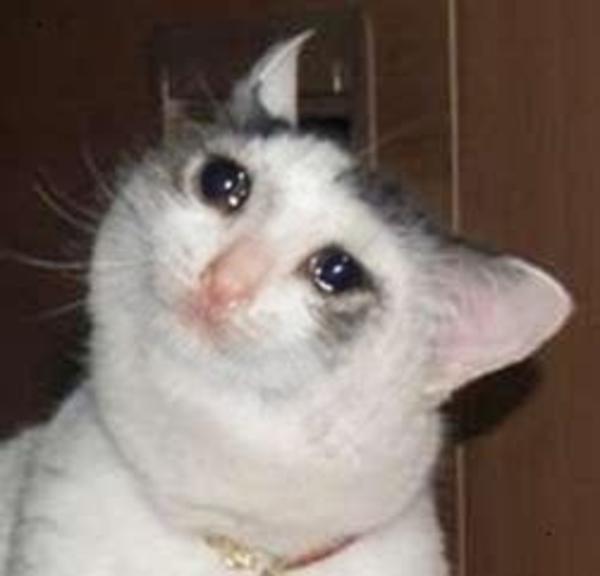
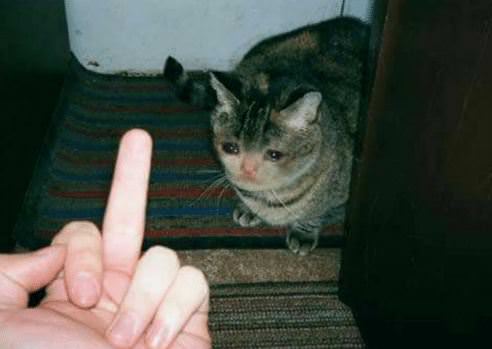
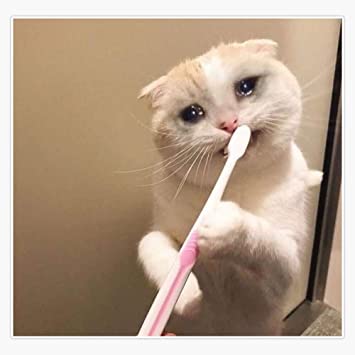
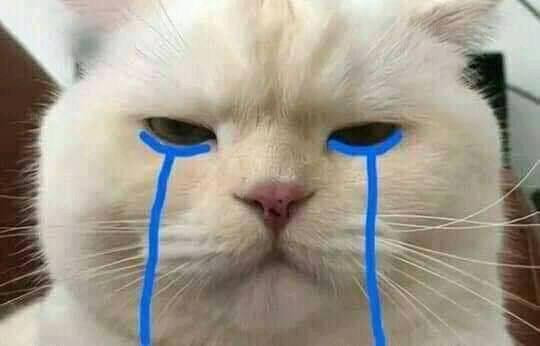
Meme mèo khóc cũng vậy khi có rất nhiều ảnh mèo được ghép với đôi mắt ngấn lệ. Hoặc đơn giản chỉ là với biểu cảm hơi buồn của chúng, bạn có thể vẽ và dòng lệ trên mắt chúng và biến nó thành meme mèo khóc. Hoặc đơn giản có thể chọn ảnh mèo khóc, meme mèo khóc ở dưới đây.
Meme mèo khóc, mèo khóc meme hài hước nhất
Bạn có thể bấm trực tiếp vào các meme mèo khóc ở dưới đây và chọn lưu lại trên album ảnh điện thoại của mình.


















Vốn là một loài động vật gần gũi nhưng cũng rất "chảnh chó" với con người. Tuy không thể hiện cảm xúc nhiều như chó nhưng mèo cũng là loài động vật hay làm ra vẻ rất là "trịch thượng" và đôi khi cũng hay giận dỗi con sen của chúng. Nhất là khi chúng tỏ ra tức giận, đôi mắt của chúng với những cái lườm sắc lẹm cũng khiến những người xung quanh cảm thấy rất giải trí và hài hước.
Meme là gì?
Internet meme, hoặc còn gọi đơn giản là meme (phát âm là mim), là các ý tưởng, hành vi, hình ảnh hay phong cách được lan truyền trên Internet, thường là thông qua những nền tảng mạng xã hội như Facebook, Messenger, Twitter, Instagram, v.v.

Những gì được coi là meme có thể sẽ khác nhau giữa những cộng đồng khác nhau trên Internet, đồng thời chúng có thể thay đổi theo thời gian. Theo truyền thống, meme là một khái niệm hoặc câu cửa miệng. Nhưng theo thời gian chúng đã thay đổi, trở nên rộng và đa nghĩa hơn, phát triển và trở thành ảnh, ảnh gif hay thậm chí là video.
Các meme được coi là một phần văn hóa của Internet. Chúng có thể lan truyền rộng rãi từ người này qua người khác qua mạng xã hội, forum, blog, tin nhắn hoặc các nguồn tin tức. Ví dụ như meme anh chàng Mohammad Akhtar chống nạnh tỏ vẻ thất vọng khi thủ môn đội bóng Pakistan mà anh hâm mộ bắt trượt cú sút của các cầu thủ Australia.
Hình ảnh của anh được lan truyền mạnh mẽ trên khắp mạng Interner ở nhiều quốc gia. Những người sử dụng meme này để thay cho lời thất vọng của họ về một điều gì đó, hoặc một sự việc nào đó mà họ biết trên Internet.
Xem thêm: