999+ Hình nền điện thoại 4K cực sắc nét, độc đáo và đẹp nhất 2024 cho dân văn phòng
Tổng hợp 500+ hình nền điện thoại cute đẹp và độc đáo phù hợp cho mọi đối tượng, cùng lựa chọn mẫu ảnh đẹp nhất cho điện thoại nhé!
Cuộc sống công sở bận rộn khiến bạn đôi khi cảm thấy nhàm chán và mệt mỏi? Hãy để hình nền điện thoại 4K trở thành liều thuốc tinh thần giúp bạn thư giãn và lấy lại cảm hứng. Những hình ảnh đẹp mắt sẽ giúp bạn giảm stress, tăng cường năng suất làm việc và tạo ra một không gian làm việc chuyên nghiệp nhưng vẫn đầy màu sắc.
Hình nền điện thoại 4K anime
Dù ai nói ngả nói nghiêng lòng ta vẫn mãi mê anime mà thôi!!! Còn chờ gì mà không tô điểm cho chiếc điện thoại của mình với những hình nền điện thoại theo phong cách truyện tranh Nhật Bản mà bạn yêu thích? Dưới đây là 15 hình ảnh anime mà chắc hẳn otaku nào cũng sẽ yêu thích.

Một chiếc hình nền vừa đáng yêu vừa huyền ảo cho bạn nữ

Một bộ phim đã lấy đi nước mắt của biết bao khán giả

Hình ảnh lãng mạn cùng với lời tuyên bố tình yêu dành mạnh mẽ của các chàng trai

Một chiếc ảnh quá lãng mạn dành cho những ai ship OTP

Hình nền điện thoại cute đậm chất manga xinh đẹp và ảo diệu

Hình ảnh hoàng hôn luôn mang đến cho ta nhiều cảm xúc

Hình nền đẹp cho điện thoại với hình ảnh thiên nhiên phong cách truyện tranh

Ai cũng muốn có một Cánh cửa thần kỳ cho mình

Khung cảnh vào buổi chiều tà mang đến sự bình yên

Hình ảnh cơn mưa hồng dành cho những ai thích sự lãng mạn

Hình nền điện thoại chú mèo đen bên đàn bướm đầy mơ mộng

Hình ảnh góc phố nhỏ với tông màu hồng dành cho các cô nàng thích sự ngọt ngào

Hình nền điện thoại đẹp dành cho những ai thích phong cách cổ trang

Cánh đồng hoa khiến cho người ta mơ mộng





















































hinh nen dien thoai 66

hinh nen dien thoai 67

hinh nen dien thoai 68

hinh nen dien thoai 69

hinh nen dien thoai 70
hinh nen dien thoai 71

hinh nen dien thoai 72

hinh nen dien thoai 73

hinh nen dien thoai 74

hinh nen dien thoai 75

hinh nen dien thoai 76

hinh nen dien thoai 77

hinh nen dien thoai 78

hinh nen dien thoai 79

hinh nen dien thoai 80

hinh nen dien thoai 81

hinh nen dien thoai 82

hinh nen dien thoai 83

hinh nen dien thoai 84

hinh nen dien thoai 85

hinh nen dien thoai 86

hinh nen dien thoai 87

hinh nen dien thoai 88

hinh nen dien thoai 88 1

hinh nen dien thoai 89

hinh nen dien thoai 90

hinh nen dien thoai 91

hinh nen dien thoai 92

hinh nen dien thoai 93

hinh nen dien thoai 94
hinh nen dien thoai 95

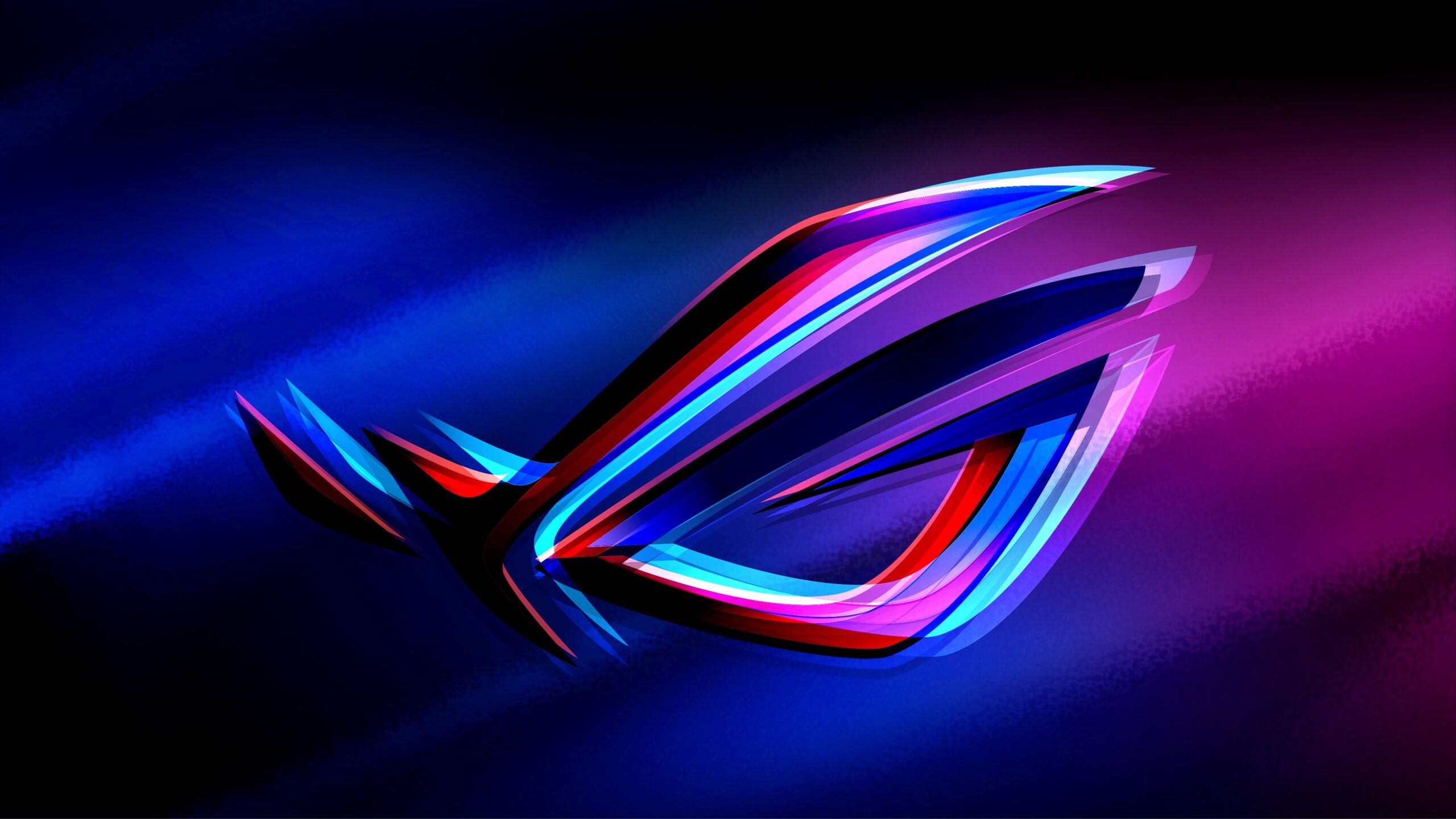
Hình nền gaming 4K cho điện thoại
Game không chỉ đơn thuần là game, mà đôi khi nó còn là nơi thỏa sức đam mê, học hỏi và kết nối với mọi người. Sử dụng hình nền điện thoại phong cách gaming 4k cũng là một trong những cách thể hiện đam mê đối với các game thủ.

Hình nền điện thoại 4k dành cho các game thủ

Hình nền điện thoại chất cho những ai đam mê hành động

Bức ảnh thể hiện cá tính mạnh của người sử dụng

Hình nền điện thoại không máu lửa đời không nể

Hình ảnh vẫn tiến về phía trước dù cô độc

Hình nền điện thoại 3d này có phải là mô phỏng cuộc sống hàng ngày của các game thủ?

Hình ảnh phi hành gia được nhiều người yêu thích

Ảnh hình nền điện thoại dành cho fan chân chính của PUBG
Ảnh nền hitech đậm cá tính

Một bức ảnh nói lên tất cả

Một thế giới nhiệm màu từ Minecraft?

Hình nền điện thoại đẹp ngầu này khiến bạn nghĩ đến game nào?
Tiếp nhận thông điệp tích cực mỗi khi mở điện thoại













































Hình nền 4K cho điện thoại cute
Những chiếc hình nền điện thoại đáng yêu, ngọt ngào có thể khiến cho tinh thần ta trở nên thoải mái và dễ chịu hơn. Lưu lại những hình ảnh dưới đây để thuận tiện cho việc thay đổi thường xuyên, đổi mới cho chiếc điện thoại của mình nhé.

Tải hình nền điện thoại cute chú mèo giữa những đám mây bồng bềnh


Nhóm bạn nhí nhố này sẽ giúp điện thoại bạn thêm phần “kawaii”

Một nụ cười luôn hé sẽ khiến ta luôn hạnh phúc

Một cốc trà cho mỗi ngày đều ngọt ngào

Khung cảnh màn đêm lung linh, lấp lánh giúp người dùng cảm thấy thư giãn hơn

Khung cảnh hoàng hôn dành cho những nàng thích sự lãng mạn

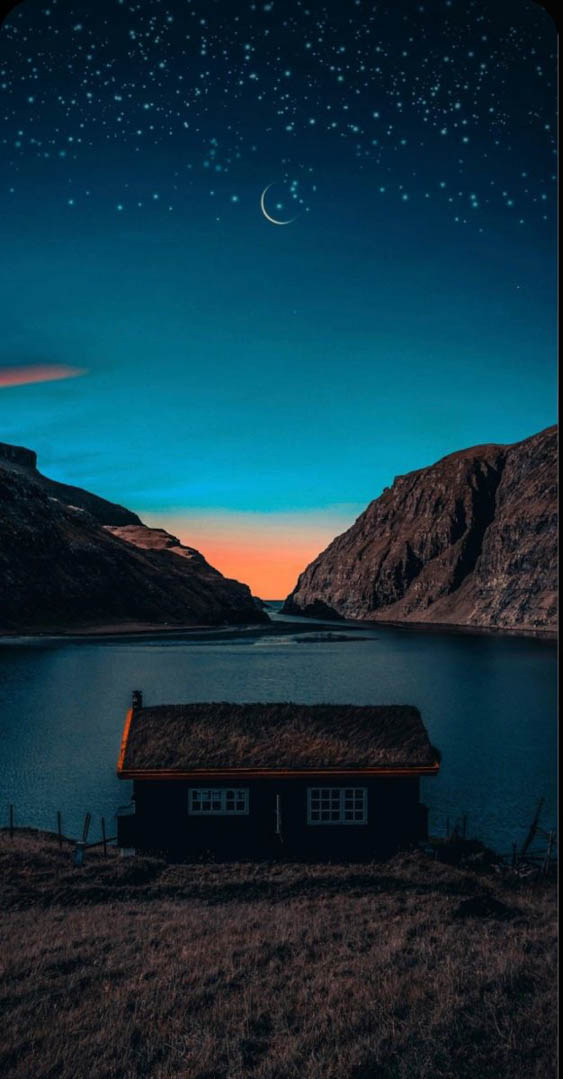
Hình nền điện thoại về màn đêm yên bình

Hình nền điện thoại OTP nhà ai đây?
Hình nền điện thoại iphone vừa dễ thương vừa chứa đựng “thông điệp” sắc bén


Hình nền cute cho điện thoại của các bạn gái

Có ai thích những bé mèo mũm mĩm đáng yêu này không?

Có ai muốn ly trà sữa đáng yêu này không nào?

Chỉ cần nhìn chú chó Shiba này sẽ giúp bạn vui vẻ cả ngày

































































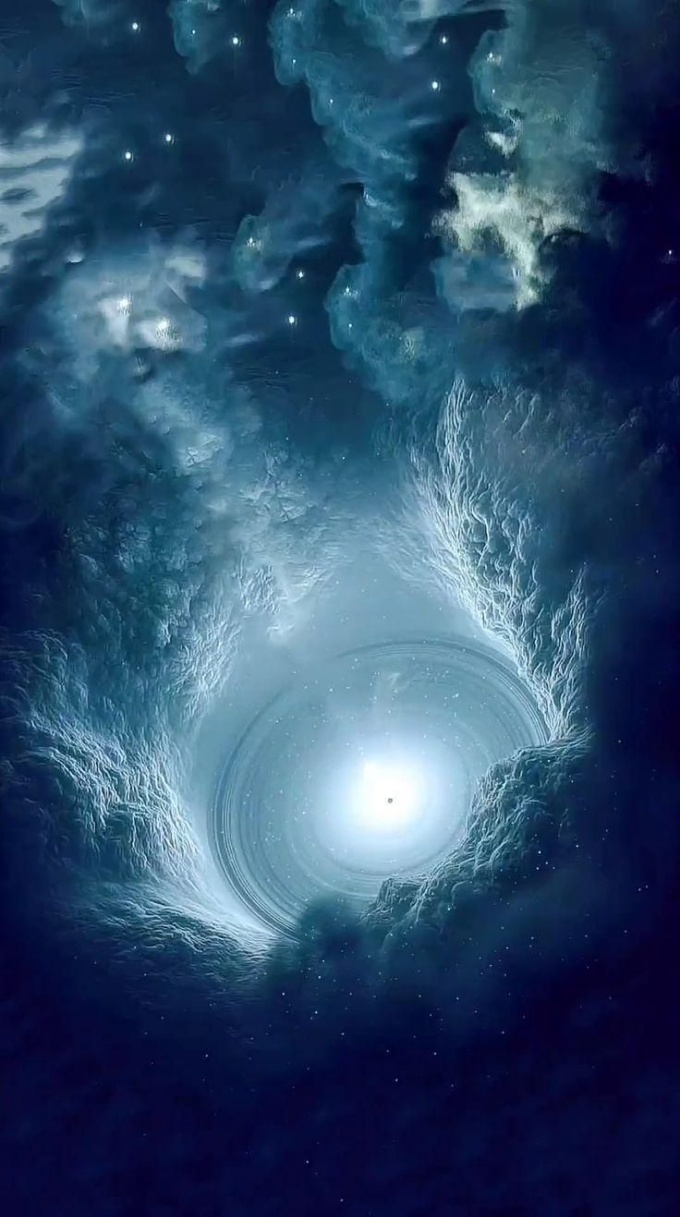
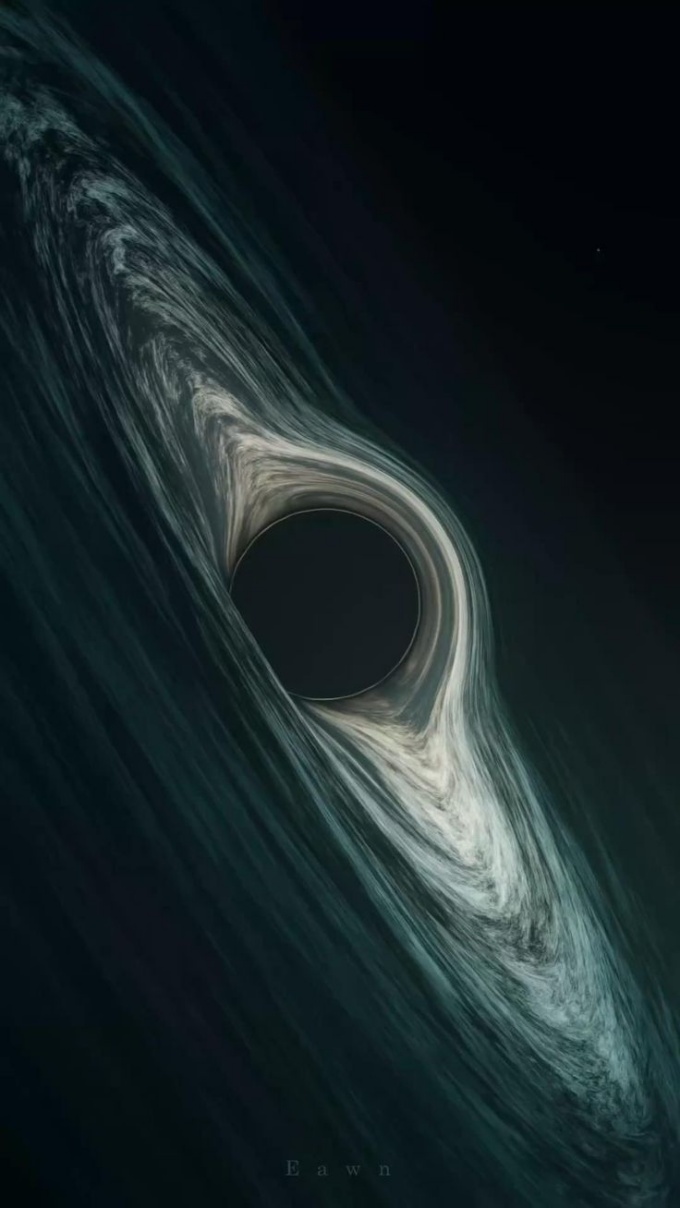
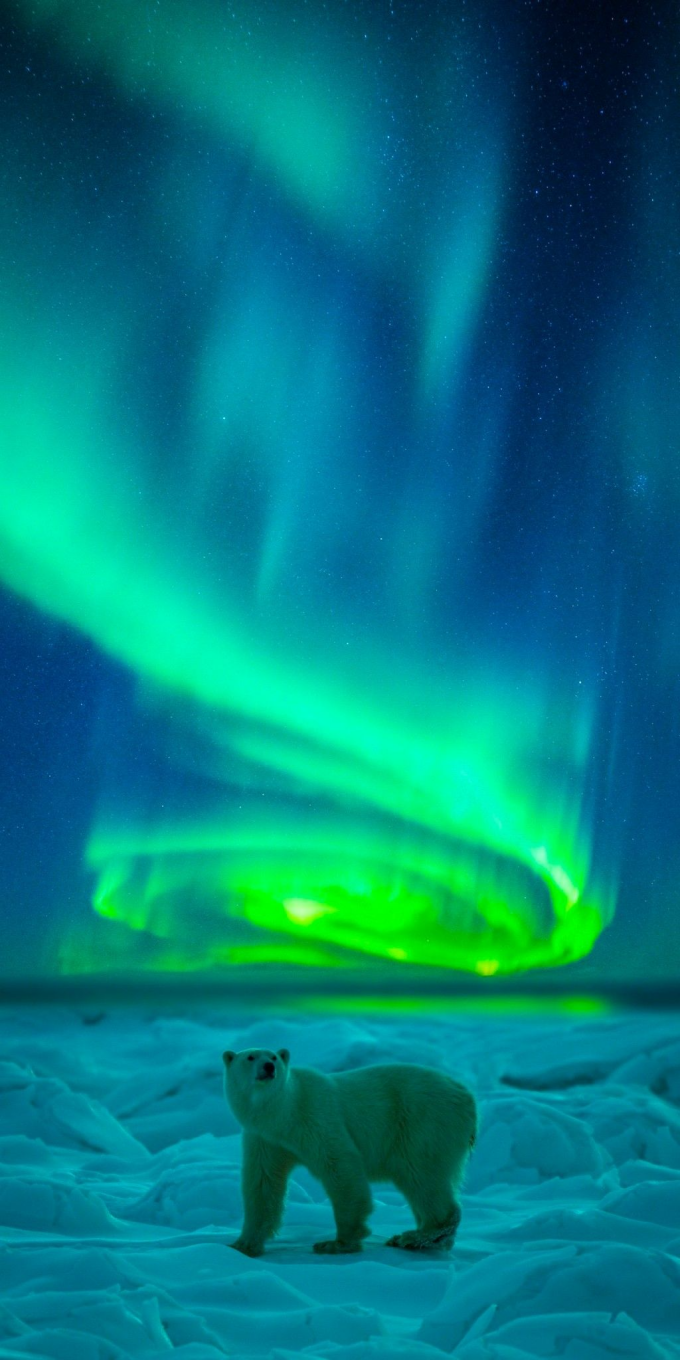
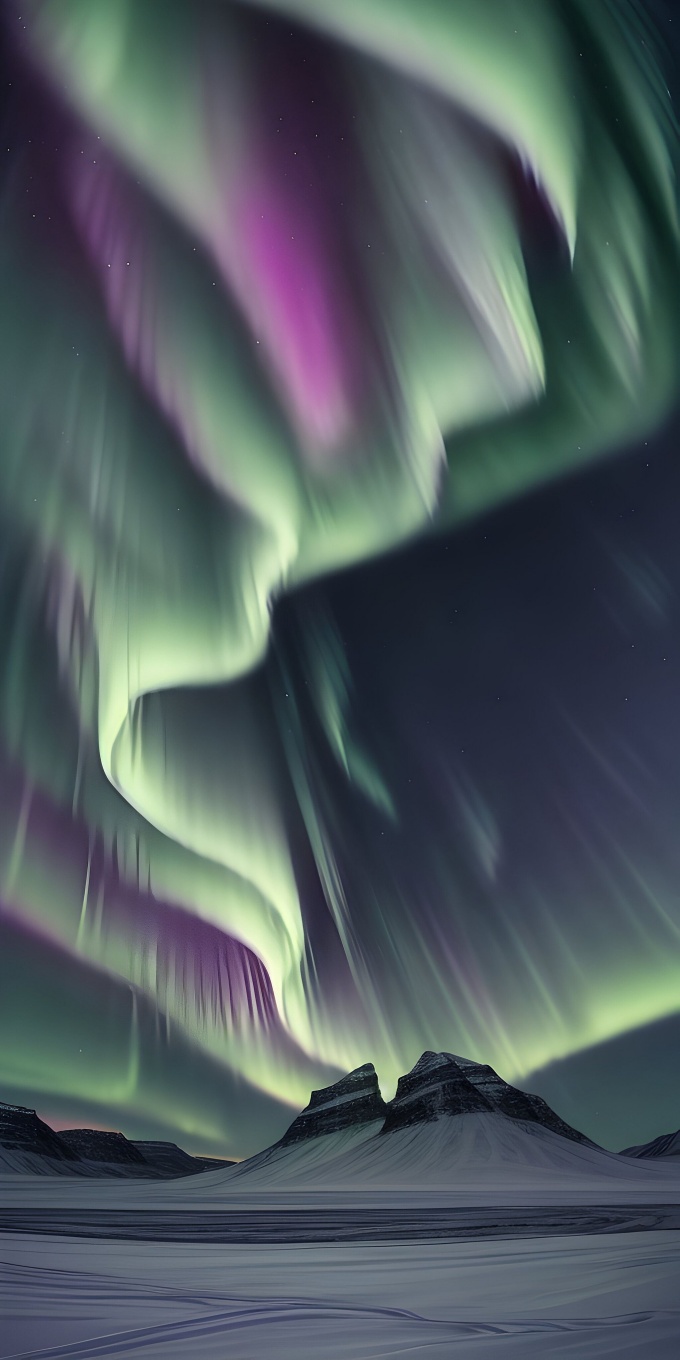
Hình nền điện thoại 4K thiên nhiên
Hình ảnh thiên nhiên hùng vĩ hay phong cảnh xanh mát sẽ làm chúng ta cảm thấy thư giãn và như được tiếp thêm năng lượng Vậy nếu bạn đang tìm cho mình những hình nền điện thoại phong cảnh 4K xinh đẹp thì hãy thử lựa chọn trong những hình ảnh dưới đây nhé.

Vượt qua đêm tối kia là hình ảnh núi non hùng vĩ

Thiên nhiên hữu tình là những gì mà chúng ta khó có thể thấy tại cuộc sống hiện đại

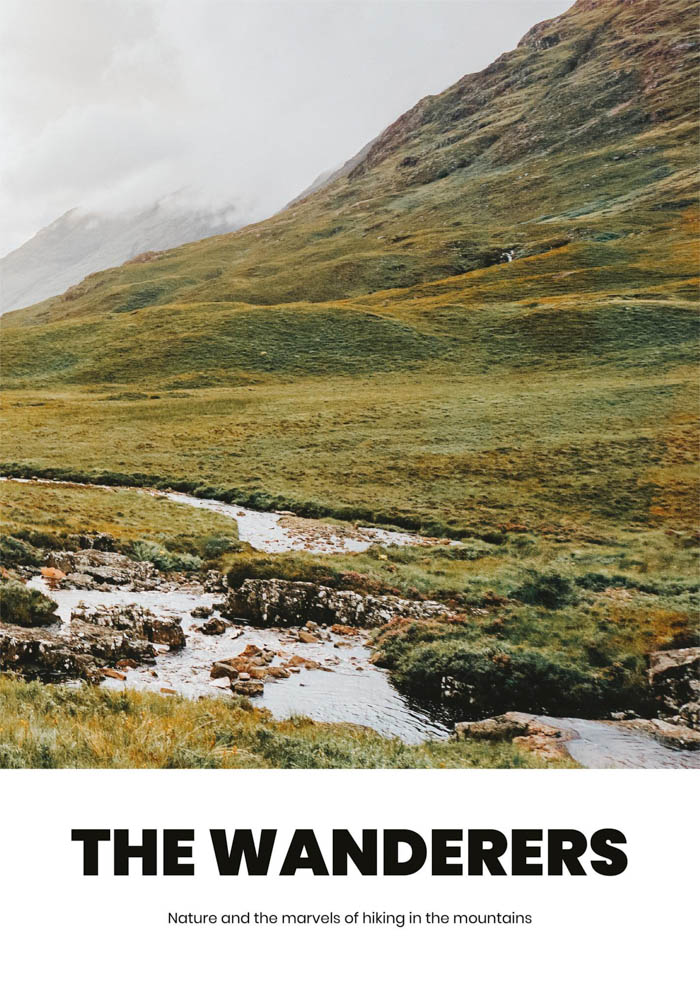
Nhìn hình ảnh này có ai muốn xách balo lên và đi không nào?

Màu xanh của cây cỏ và bầu trời luôn mang đến cảm giác thoải mái

Khung cảnh huyền ảo khiến ai cũng muốn đặt chân đến dù chỉ một lần

Khung cảnh cực quang đầy ảo diệu và huyền bí

Khung cảnh có màu trầm phù hợp cho những ngày tâm trạng

Khung cảnh bình yên khiến ta muốn quay trở về với tuổi thơ

Hình nền điện thoại giúp ta nhìn thấy sự vĩ đại của thiên nhiên
Hình nền điện thoại đơn giản nhưng được nhiều người ưa thích

Hình nền điện thoại đẹp nhất hiện nay về phong cảnh

Hình nền 4k cho điện thoại với cánh đồng xanh mướt đầy yên bình

Hình ảnh tòa lâu đài như trong các câu chuyện cổ tích ta thường đọc

Cánh đồng tuyết dưới cực quang? Có ai muốn được đặt chân đến đây khám phá không?

Bầu trời đêm ngàn sao cho những ai thích sự lãng mạn






































































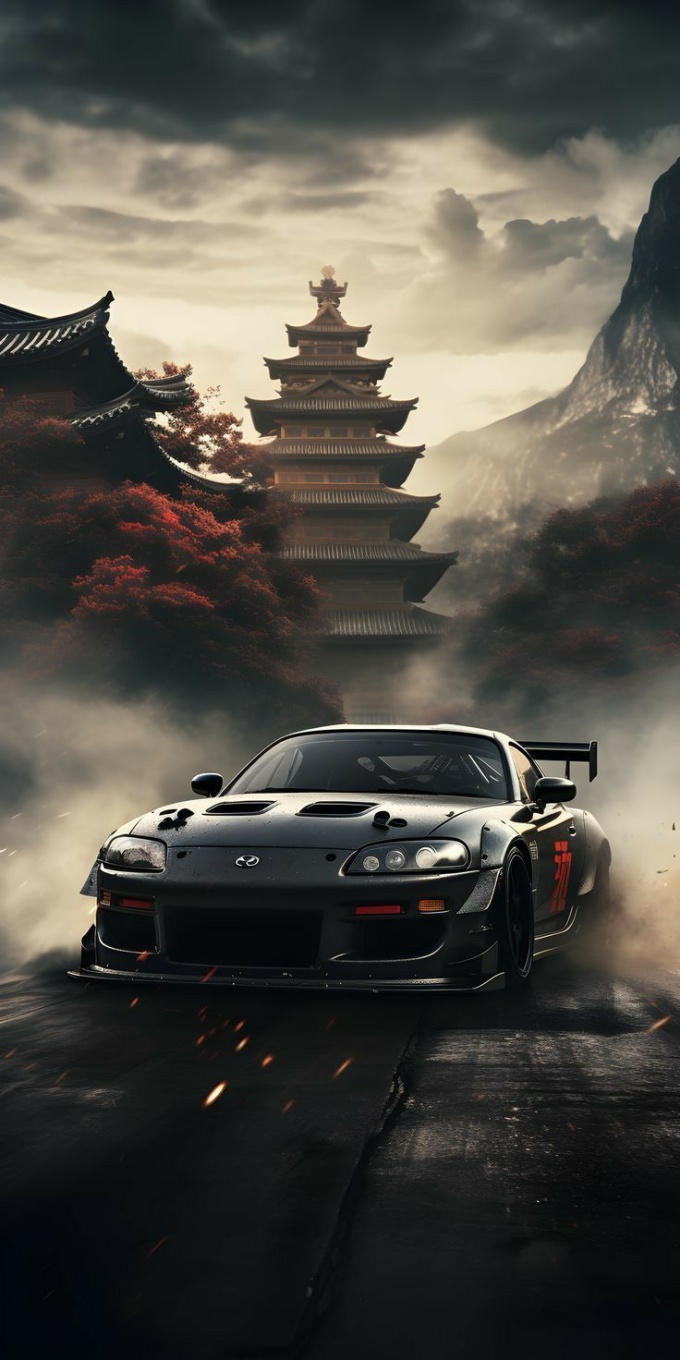
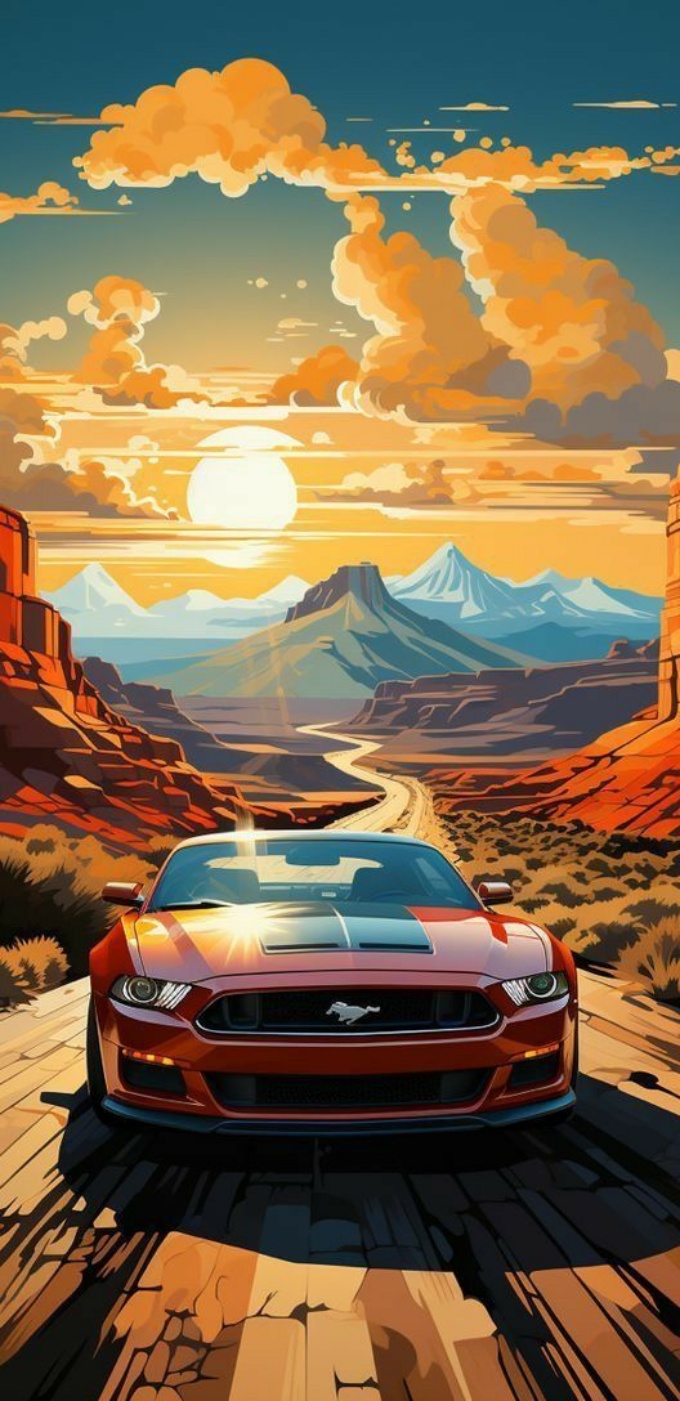
Hình nền 4K siêu xe cho điện thoại



































































Hình nền điện thoại 4K iphone
Bạn muốn đổi mới cho chiếc iphone của mình khỏi hình ảnh mặc định có phần nhàm chán và dễ bị “đụng hàng” với nhiều người? Hãy thử những hình nền điện thoại xinh xắn, sinh động và được nhiều người yêu thích dưới đây nhé.

Bạn có từng muốn ngắm mưa sao băng?

Tranh Van Gogh kết hợp Totoro, tại sao không?
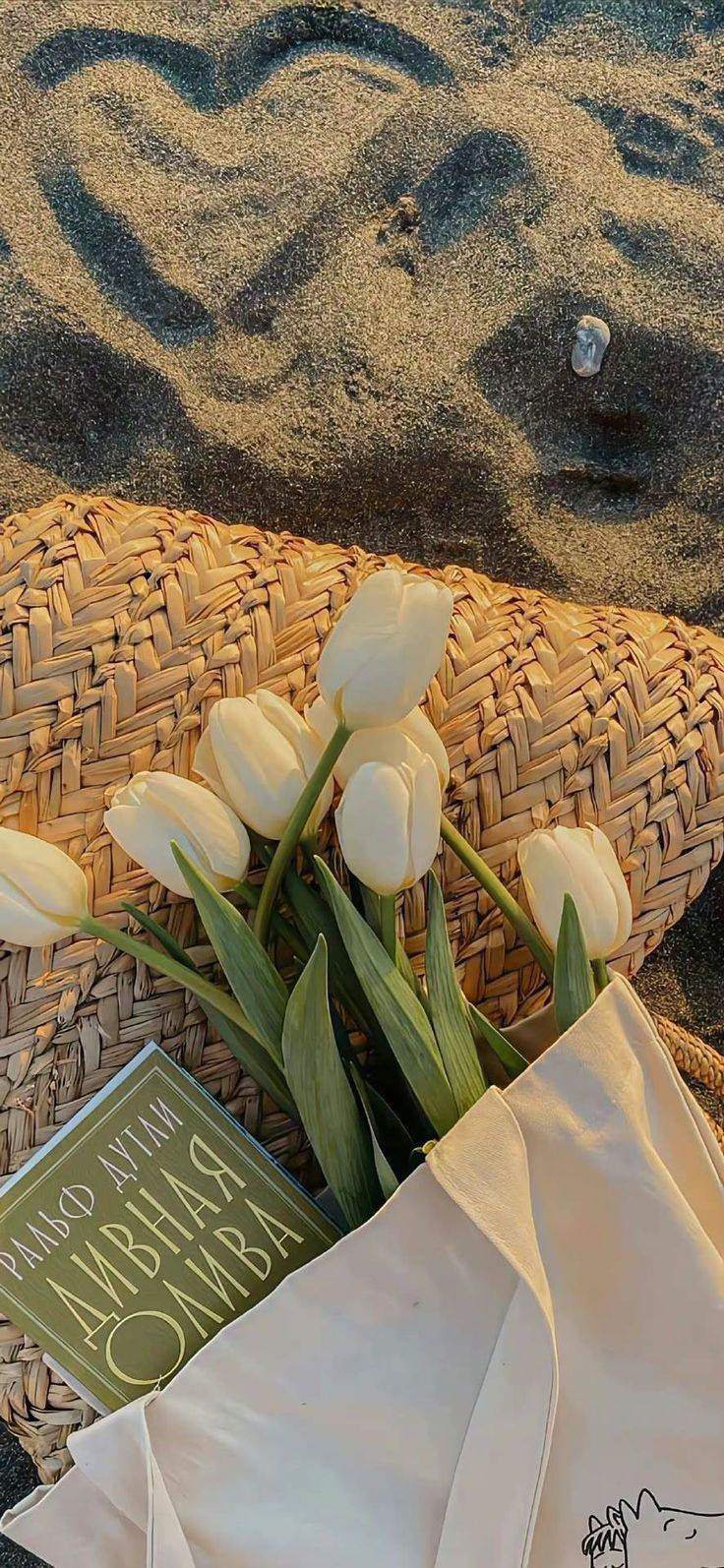
Một đóa hoa dành cho những nàng nhẹ nhàng

Khung cảnh thiên nhiên gợi mở khát khao khám phá

Khung cảnh bình minh trên biển biết bao yên bình

Hình nền điện thoại tượng trưng cho vẻ đẹp có thể xuất hiện bất cứ lúc nào

Hình nền điện thoại nhắn gửi lời chào mỗi ngày cho bạn
Hình nền điện thoại iphone mang theo thông điệp tích cực
Hình nền điện thoại đơn giản nhưng không mất đi sự tinh tế

Hình nền dành cho những người thích phong cách tối giản

Hình ảnh vừa lãng mạn vừa sâu lắng cho những ai thích ảnh “deep”

Hình ảnh thiên nhiên được nhiều người ưa chuộng

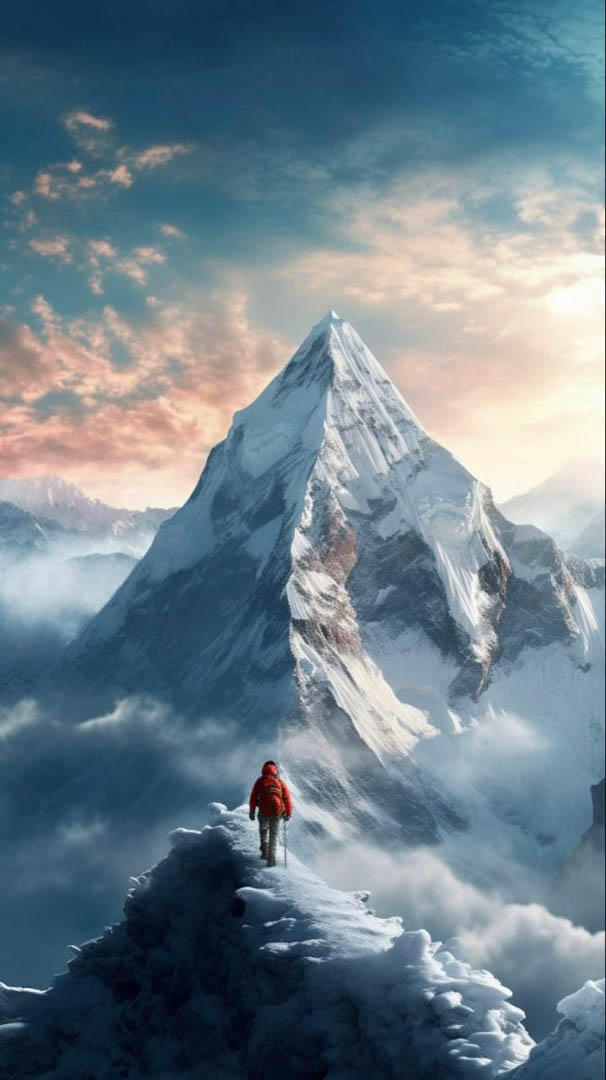
Đỉnh núi Everest tượng trưng cho giấc mơ chinh phục đỉnh cao

Biểu tượng Apple với phong cách mới lạ hơn
Thông điệp sắc bén dành cho những ai đang có “ý đồ” với điện thoại bạn

























































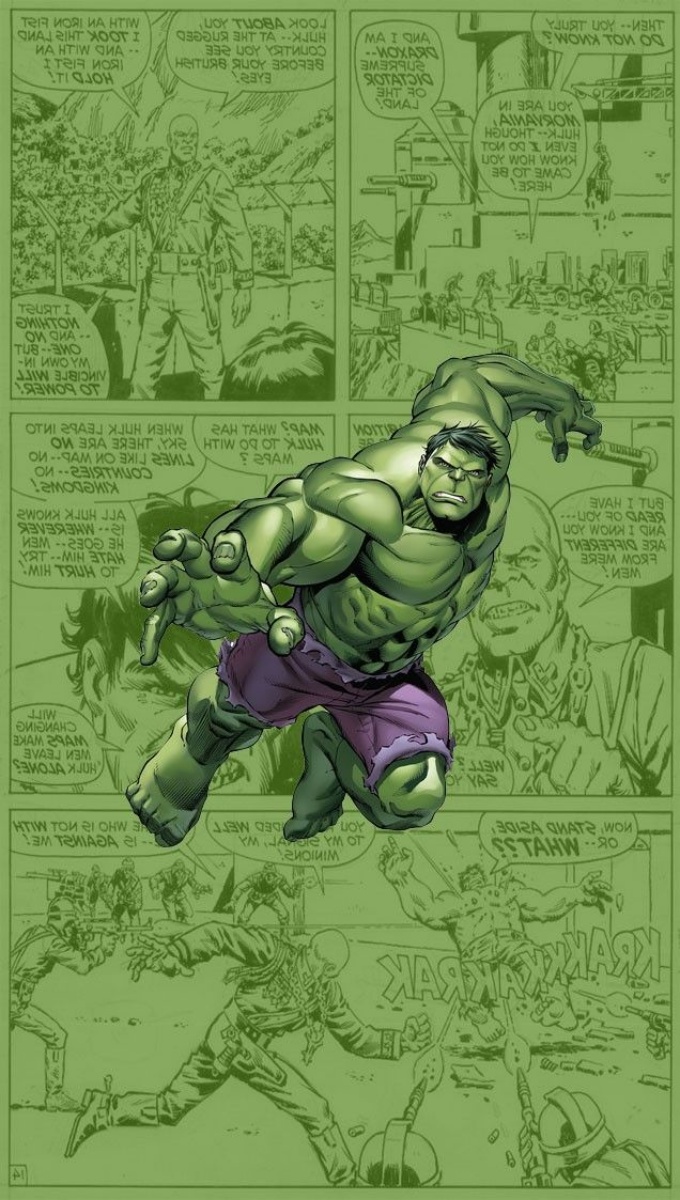
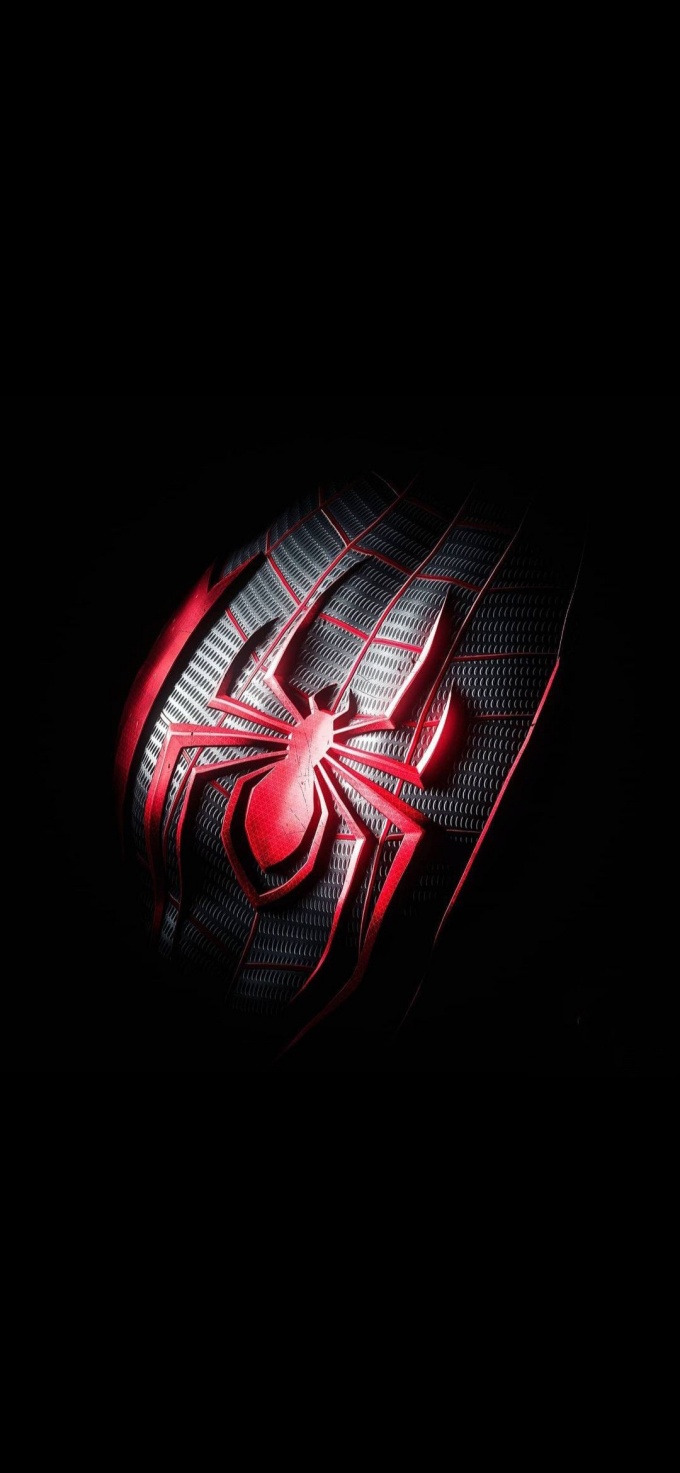
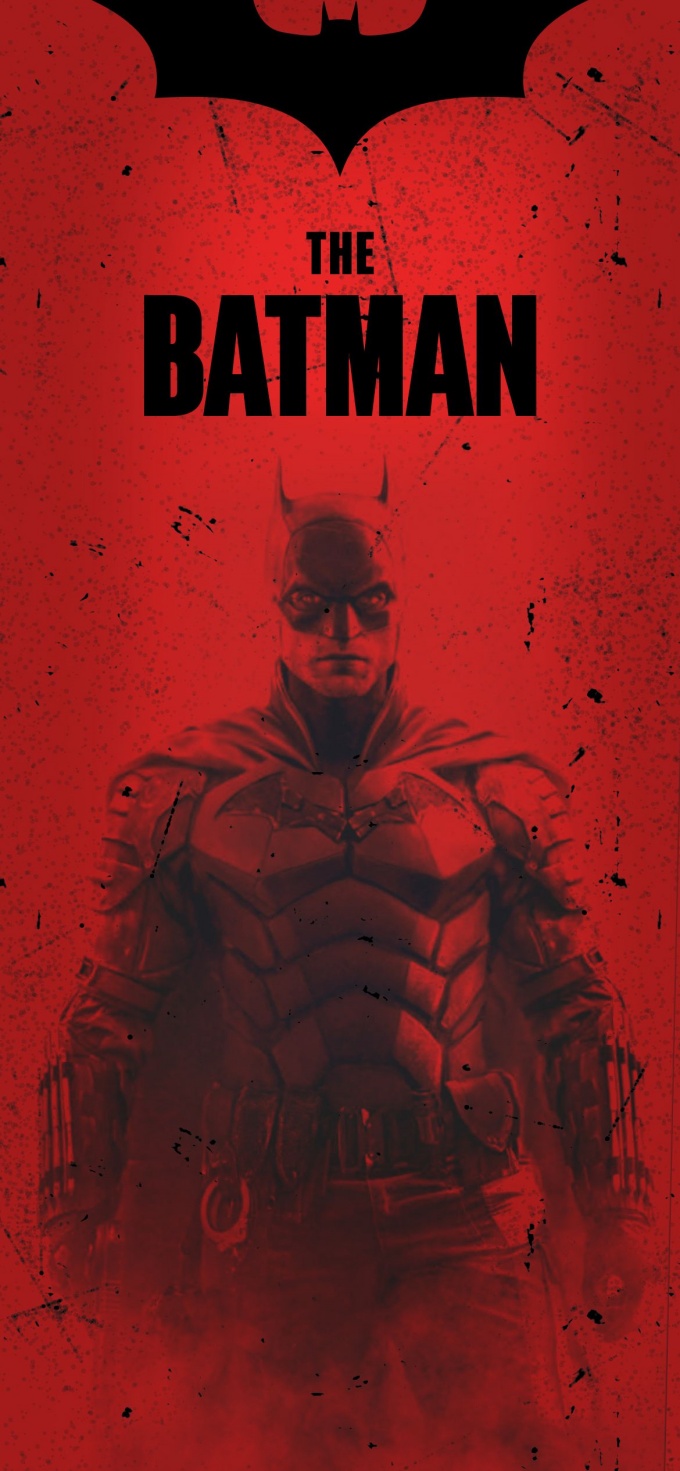
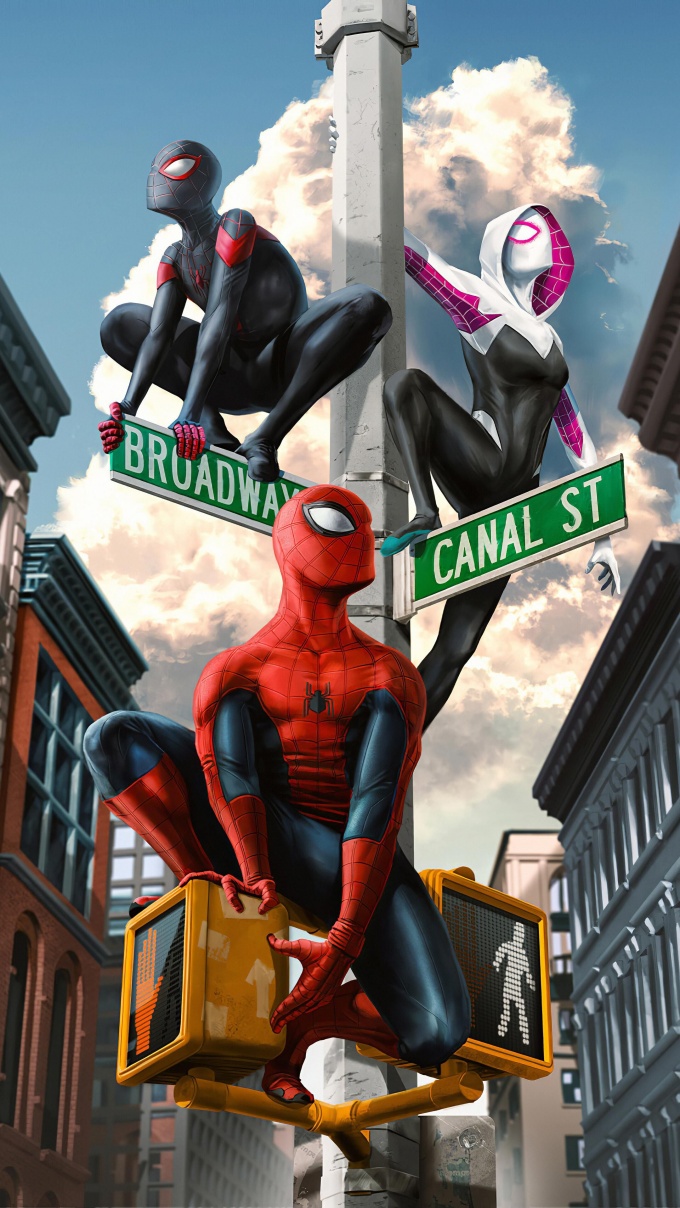
Hình nền điện thoại siêu anh hùng












































































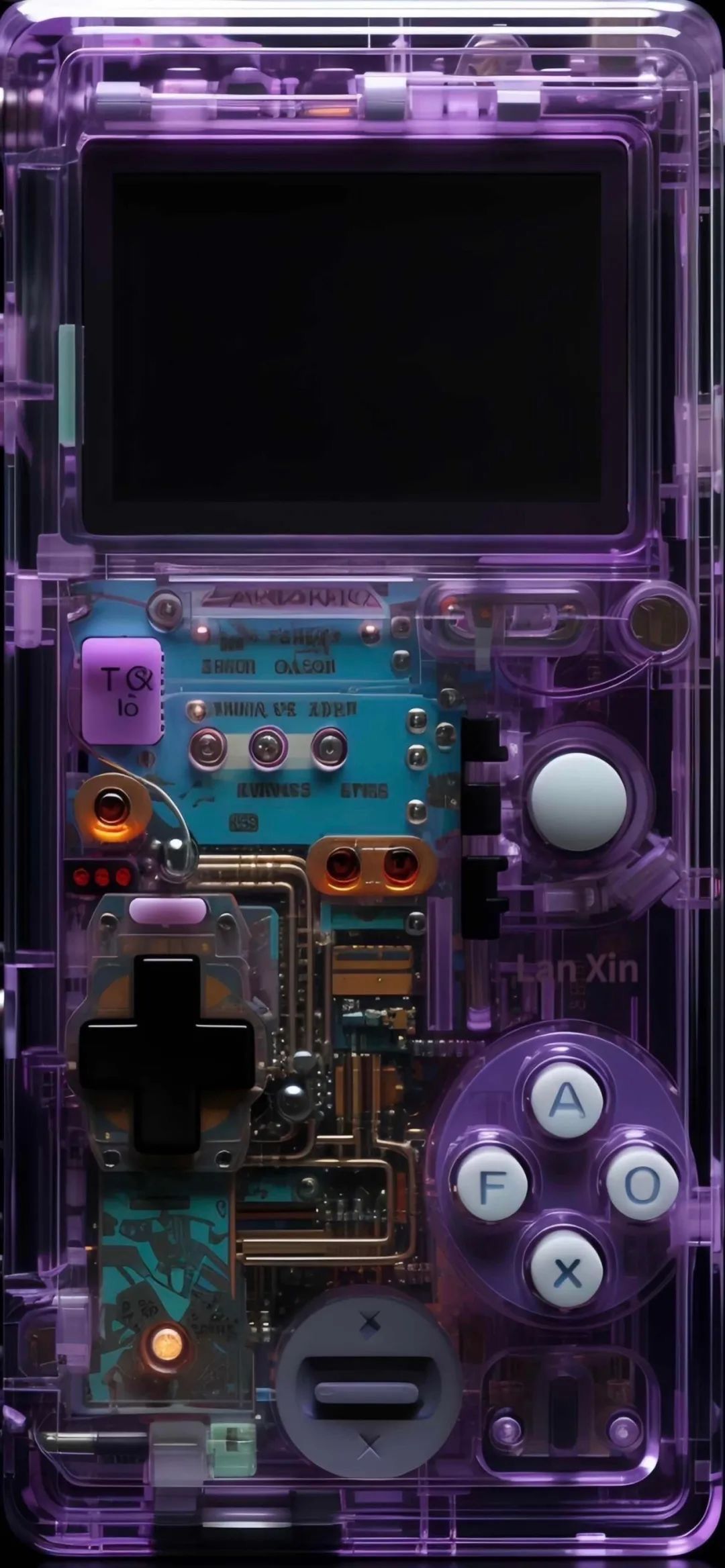
Hình nền điện thoại 4K công nghệ
Là một người đam mê công nghệ, IT thì không thể nào bỏ qua những hình nền công nghệ đậm cá tính và siêu xịn sò này. Cùng lựa chọn và làm mới giao diện cho điện thoại của mình nhé.

Tông màu cam ấm nóng tượng trưng cho sự nhiệt huyết, máu lửa

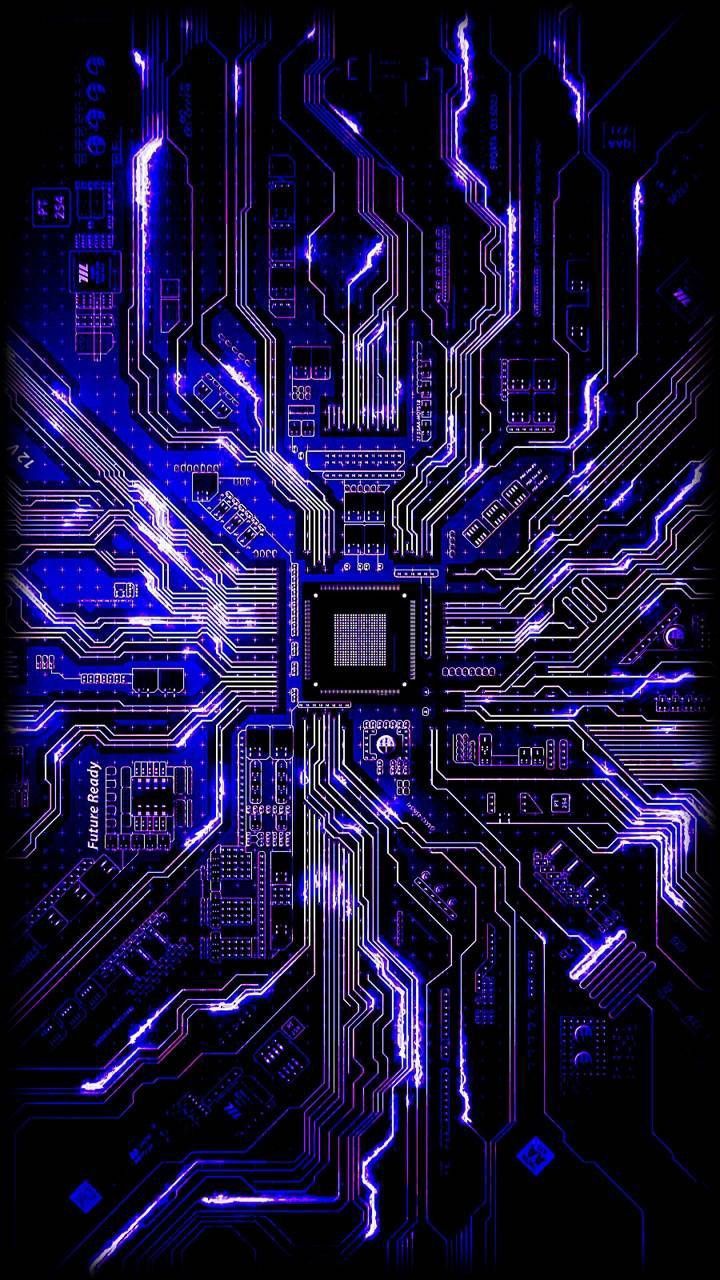
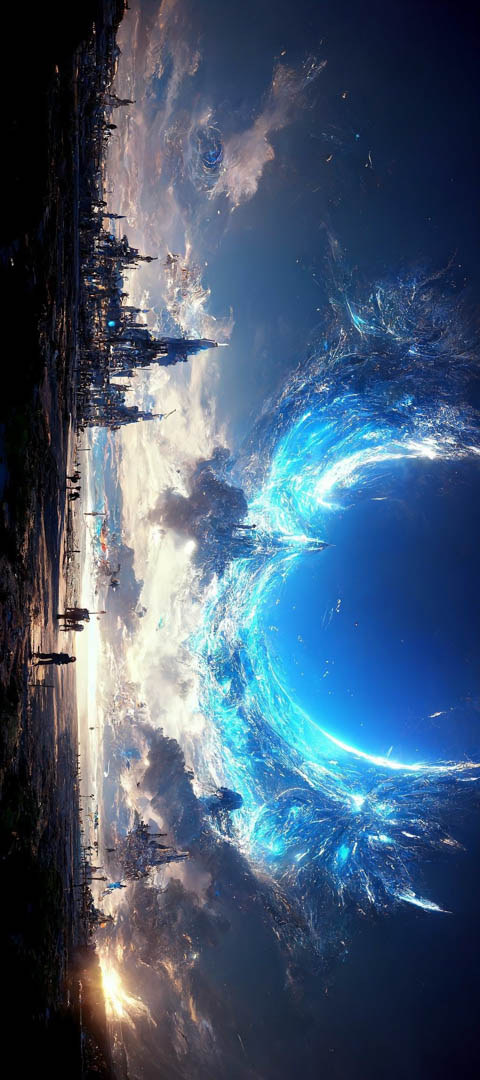
Thế giới ảo chứa đựng biết bao điều bí ẩn
Sự bí ẩn, khơi gợi mong muốn khám phá khiến nó được nhiều người ưa chuộng
Nhìn hình ảnh này bạn nghĩ đến điều gì?
Một bộ máy xịn là ước mơ của biết bao người

Hình nền màu đen thể hiện sự sang trọng và tinh tế

Hình nền hightech màu đen mang đến cảm giác tinh tế và sang trọng
Hình nền điện thoại về công nghệ theo phong cách đơn giản

Hình nền điện thoại tối giản những thể hiện sự yêu thích công nghệ của người dùng

Hình nền điện thoại công nghệ cho các bạn nam
Hình nền công nghệ đầy cá tính

Hình ảnh trí tuệ nhân tạo được nhiều người quan tâm hiện nay
Hình ảnh kết hợp giữa màu tối và sáng giúp điện thoại bạn thêm màu sắc
Đây có thể sẽ là hình nền điện thoại được các IT boy yêu thích
Công nghệ thì không thể thiếu những cánh tay robot đắc lực
Hình nền điện thoại về các hiện tượng siêu nhiên












































































































































Hình nền 4K các môn thể thao mạo hiểm










































































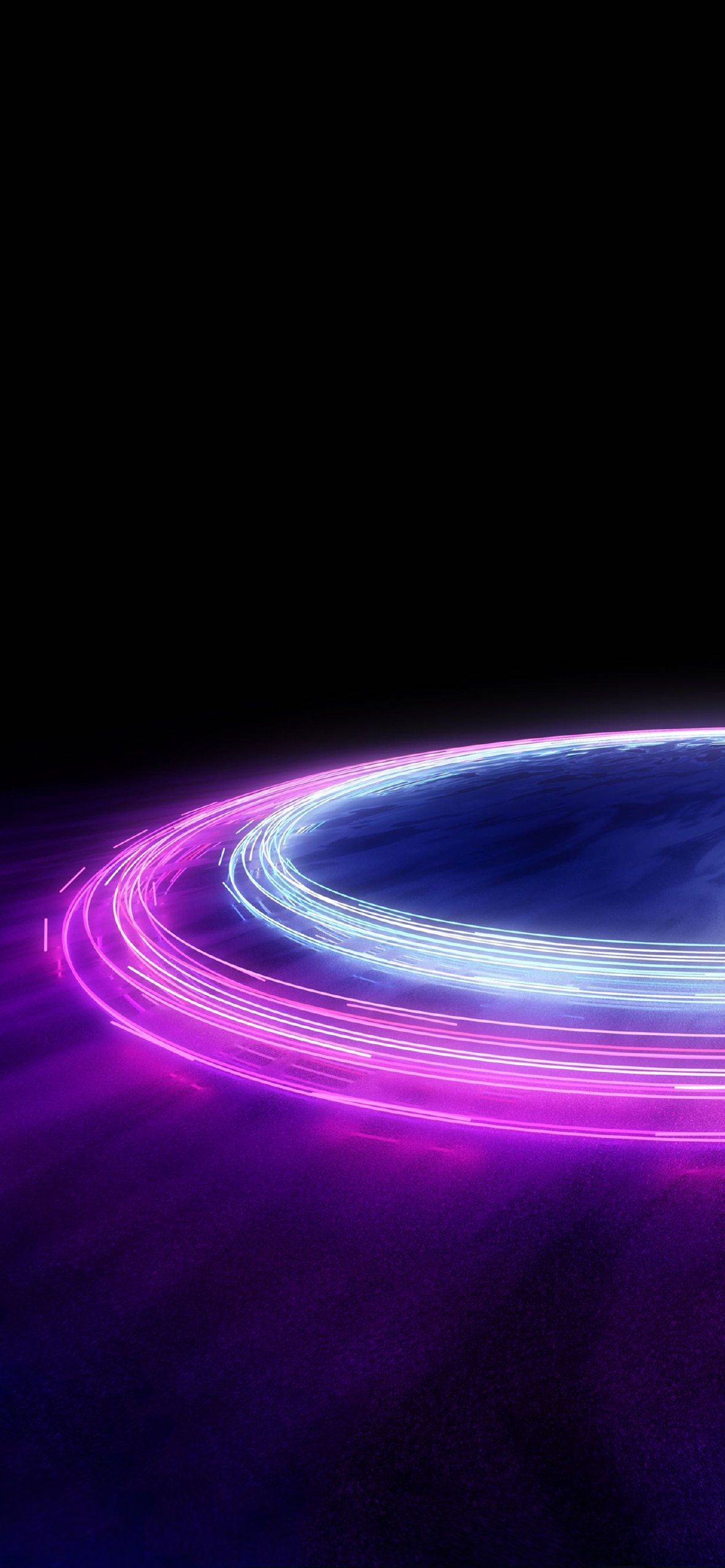
Hình nền không gian bí ẩn 4K






































































Ngoài ra chủ để caption đăng MXH cũng được nhiều người quan tâm
- Những câu nói hay về cuộc sống nổi tiếng
- Caption hay về cuộc sống vui vẻ thú vị
- Nhiều STT thả thính hài hước cho bạn lựa chọn
- Tất tần tật các caption hài hước đăng lên bão like
- Đọc thêm những câu nói hay về nhân cách sống






Mỗi ngày làm việc đều trở nên tươi mới hơn với một chiếc điện thoại được khoác lên tấm áo mới đầy màu sắc. Hãy để VietnamWorks HR Insider đồng hành cùng bạn tìm kiếm những hình nền điện thoại 4K độc đáo nhất, giúp bạn thư giãn và lấy lại năng lượng sau những giờ làm việc căng thẳng. Còn chần chừ gì nữa, hãy khám phá ngay kho tàng hình nền khổng lồ mà chúng tôi chia sẻ trên đây nhé!
> Xem thêm:
- 99+ Bộ Hình Nền Máy Tính Full HD Đẹp Độc Nhất Vô Nhị
- Trọn bộ Ảnh Anime Cute Siêu ĐángYêu
- Top hình ảnh thiên nhiên 3D đẹp chất lượng
- Những hình vẽ cute đáng yêu nhất
- Các hình xăm tay phổ biến hot
- Bộ hình ảnh đại diện Facebook ý nghĩa
— HR Insider—
VietnamWorks – Website tuyển dụng trực tuyến số 1 Việt Nam
ĐĂNG KÝ TÀI KHOẢN TÌM VIỆC
VietnamWorks là nền tảng tuyển dụng trực tuyến lớn nhất Việt Nam, với hơn 20 năm kinh nghiệm và hàng triệu ứng viên tiềm năng. VietnamWorks kết nối hiệu quả người tìm việc với các nhà tuyển dụng uy tín trên mọi lĩnh vực, giúp người tìm việc nhanh chóng tìm được công việc mơ ước. Tại VietnamWorks, người tìm việc sẽ được truy cập hàng ngàn tin tuyển dụng mới nhất, cập nhật liên tục từ các doanh nghiệp hàng đầu, tìm kiếm việc làm phù hợp với năng lực, kinh nghiệm và sở thích. Ứng tuyển dễ dàng chỉ với vài thao tác đơn giản. Đặc biệt, người tìm việc làm có thể tạo CV trực tuyến miễn phí, chuyên nghiệp và thu hút nhà tuyển dụng và nhận gợi ý việc làm phù hợp dựa trên CV và kinh nghiệm, để tìm việc nhanh chóng tại môi trường làm việc mơ ước.
Post Views: 329,994
Admin
Link nội dung: https://pi-web.eu/999-hinh-nen-dien-thoai-4k-cuc-sac-net-doc-dao-va-dep-nhat-2024-cho-dan-van-phong-1735800315-a2618.html