Bức ảnh đại diện cặp đôi, hình ảnh couple đáng yêu được giới trẻ ưa chuộng trên mạng xã hội. Trong bài viết này, Mytour mang đến những hình ảnh avt cặp đôi độc đáo nhất.

![]()
Ảnh đại diện cặp đôi dễ thương nhất (1)
![]()
Ảnh đại diện cặp đôi dễ thương nhất (2)
![]()
Ảnh Avatar đôi xinh đẹp (1)
![]()
Ảnh Avatar đôi xinh đẹp (2)

Ảnh Avt cặp đôi Anime ngọt ngào (1)

Ảnh Avt cặp đôi Anime ngọt ngào (2)

Ảnh đôi Anime dễ thương nhất (1)
Ảnh đôi Anime dễ thương nhất (2)
![]()
Hình đại diện đôi ngầu lạ mắt (1)
![]()
Hình đại diện đôi ngầu lạ mắt (2)
![]()
Ảnh Avatar đôi ngọt ngào (1)
![]()
Ảnh Avatar đôi ngọt ngào (2)
![]()
Ảnh Avatar cặp đôi dễ thương nhất (1)
![]()
Ảnh Avatar cặp đôi dễ thương nhất (2)
![]()
Ảnh Avatar đôi dễ thương nhất (1)
![]()
Ảnh Avatar đôi dễ thương nhất (2)
![]()
Ảnh Avatar đôi trẻ trung (1)
![]()
Ảnh Avatar đôi trẻ trung (2)
![]()
Ảnh Avatar đôi tết ngày lễ (1)
![]()
Ảnh Avatar đôi tết ngày lễ (2)
![]()
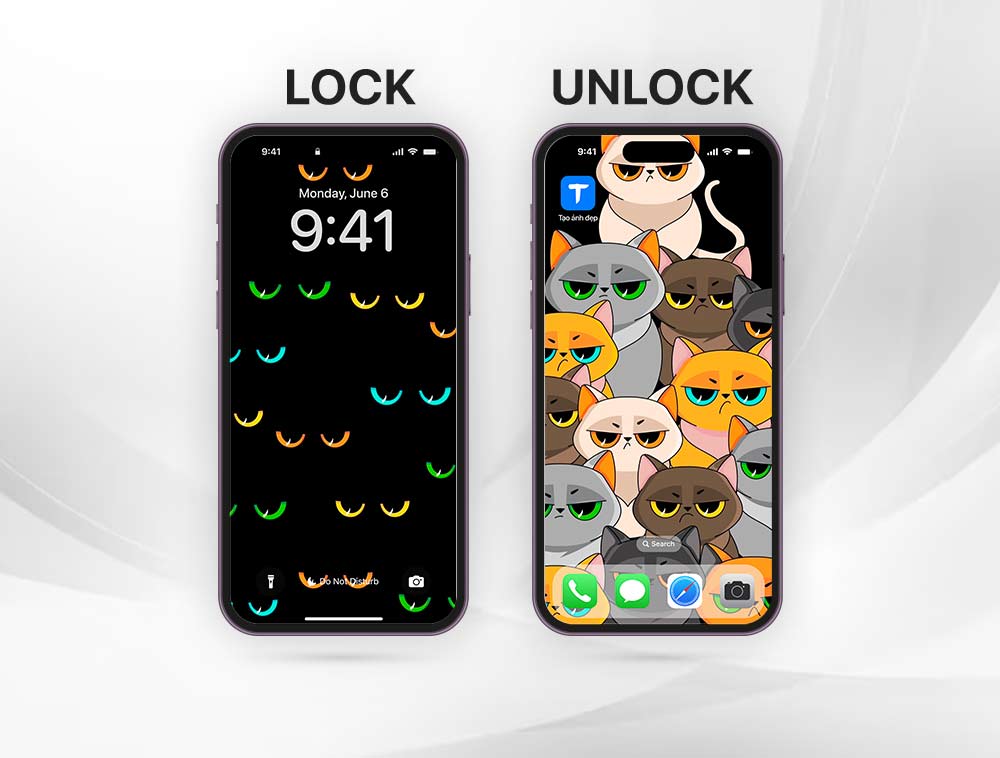
Ảnh Avatar đôi mèo dễ thương (1)
![]()
Ảnh Avatar đôi mèo dễ thương (2)

Avt anime đôi đẹp (1)

Avt anime đôi đẹp (2)

Avt đôi xinh đẹp (1)

Avt đôi xinh đẹp (2)

Avt đôi dễ thương đỉnh cao (1)

Avt đôi dễ thương đỉnh cao (2)

Avt đôi dễ thương siêu cute (1)
Avt đôi dễ thương siêu cute (2)

Avt đôi đẹp như cổ tích (1)

Avt đôi đẹp như cổ tích (2)

Avt đôi lãng mạn ngọt ngào (1)

Avt đôi lãng mạn ngọt ngào (2)

Avt đôi ngầu phong cách (1)

Avt đôi ngầu phong cách (2)

Avt đôi tình yêu mãi mãi (1)

Avt đôi tình yêu mãi mãi (2)

Avt đôi anime xinh đẹp (1)

Avt đôi anime xinh đẹp (2)

Avt đôi dễ thương ngọt ngào (1)

Avt đôi dễ thương ngọt ngào (2)

Avt mèo đôi xinh đẹp (1)

Avt mèo đôi xinh đẹp (2)

Hình ảnh Avt đôi dễ thương nhất (1)

Hình ảnh Avt đôi dễ thương nhất (2)
![]()
Hình Avatar đôi đẹp lung linh (1)
![]()
Hình Avatar đôi đẹp lung linh (2)
![]()
Hình avatar đôi cute đáng yêu (1)
![]()
Hình avatar đôi cute đáng yêu (2)
Trong bài viết này, Mytour muốn chia sẻ những hình ảnh Avatar cặp đôi đáng yêu nhất, để tạo thêm niềm vui và sự tươi mới cho ngày của bạn. Hy vọng bạn sẽ thích!
Nội dung được phát triển bởi đội ngũ Mytour với mục đích chăm sóc khách hàng và chỉ dành cho khích lệ tinh thần trải nghiệm du lịch, chúng tôi không chịu trách nhiệm và không đưa ra lời khuyên cho mục đích khác.
Nếu bạn thấy bài viết này không phù hợp hoặc sai sót xin vui lòng liên hệ với chúng tôi qua email [email protected]